Urology in the US is steadily evolving towards safer, more cost-effective, and minimally invasive procedures. A key example of this shift is the increasing adoption of the Seldinger technique for suprapubic tubing (SPT).
The Lowsley retractor is a surgical instrument that elevates the bladder during suprapubic tubing placement (SPT). This has been used for many years to help create a suprapubic tract from “the inside out” so avoids some of the issues using blind trocars, such as damaging the posterior wall of the bladder. It is passed through the urethra and pressed against the inner bladder wall, guiding the surgeon to make an incision from the outside.
The Seldinger technique is a guidewire-assisted approach used to gain controlled access to the bladder prior to inserting a sheath dilator and catheter suprapubically. It is recognized as a highly precise, safer, and less traumatic method of catheter insertion compared to blind insertion.
The adoption of the Seldinger technique signifies a vital evolution in urology care. Offering enhanced safety, greater accuracy, and improved patient comfort, this approach effectively addresses the limitations of traditional blind methods.
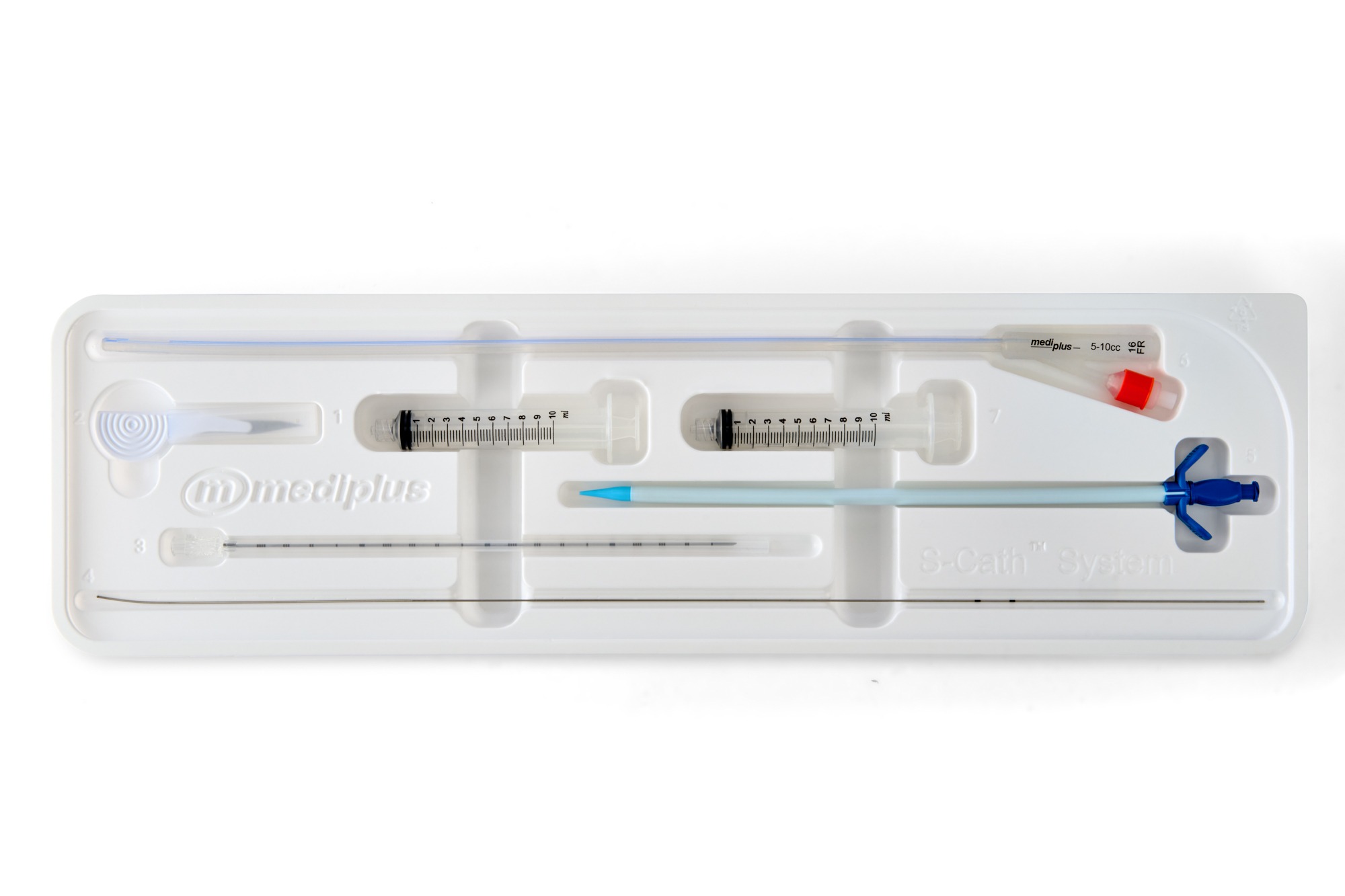
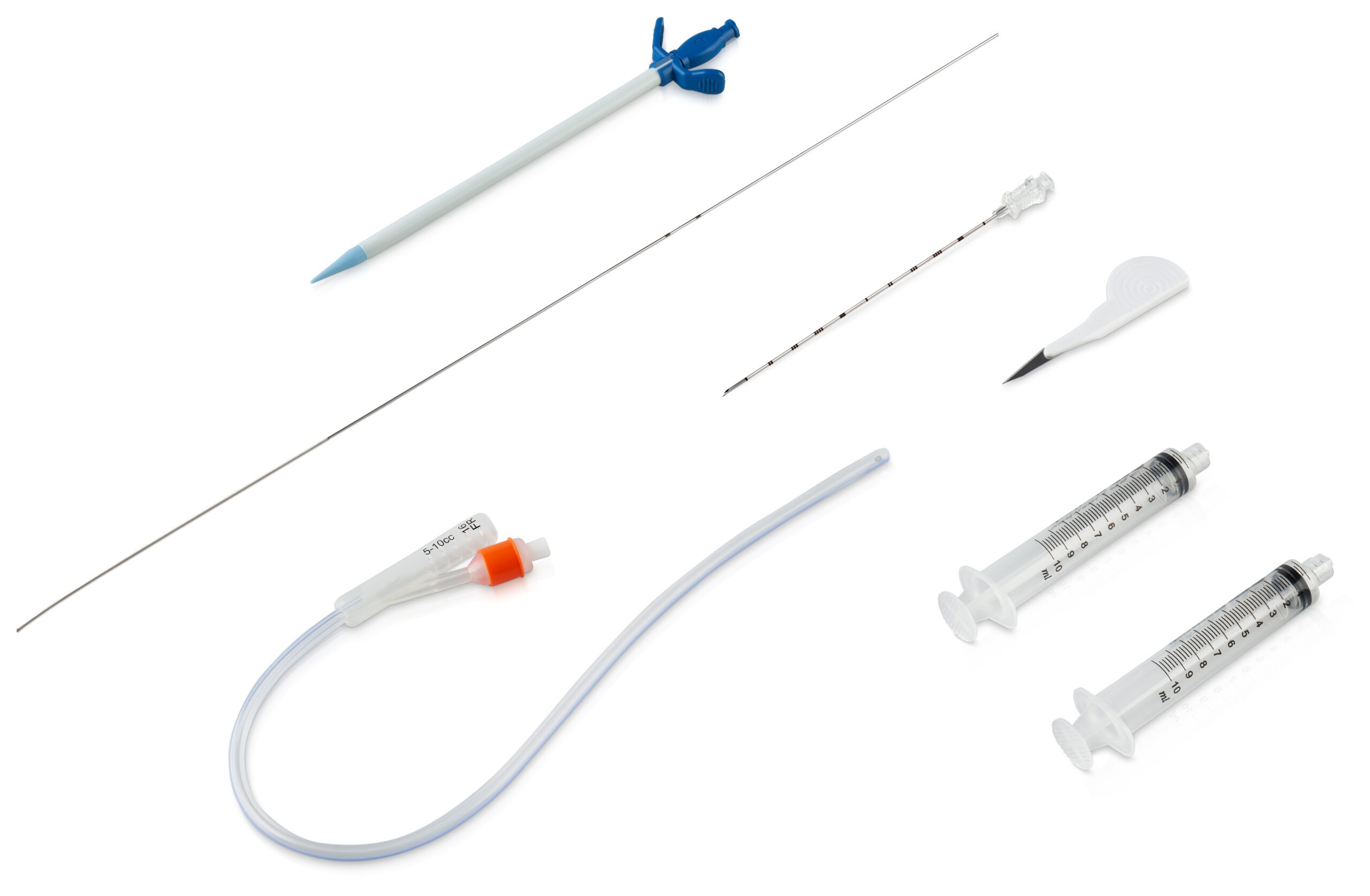
A more recent development is the S-Cath™ System. This features a patented design that employs the Seldinger technique to deliver a comprehensive, user-friendly solution to enhance the safety of suprapubic catheterization. This system reduces the need for general anesthesia, making the procedure safer and more accessible. The use of a 3-stage guidewire ensures accurate catheter placement, significantly reducing the risks associated with blind insertion. Supplied as a sterile, complete kit – including a needle, guidewire, sheath dilator, silicone Foley catheter, scalpel, and syringes—the system supports both inpatient and outpatient use across adult populations. As healthcare providers work to reduce complications and improve efficiency, advanced devices like the S-Cath™ System offer a precise, low-risk, minimally invasive SPT solution that elevates patient care.
The S-Cath™ System is available exclusively from PSS Urology in the USA.
“The kit itself is robust and of good quality, and I would strongly recommend its use in all urology, gynaecology, A&E, as well as in all theatre suites.”
Consultant Urological Surgeon
The Freeman Hospital
To order a sample, arrange a training session, or speak to a product specialist click the button below.

References: